The High Risk Personality Programme - Revised: An evaluation report
Dr Nick Wilson
Glen Kilgour
Principal Adviser Special Treatment Unit Development, Department of CorrectionsAuthor biographies
Glen Kilgour trained as a clinical psychologist at Waikato University, graduating in the early 1990s. He has worked in the Department since 1995 in a variety of roles including principal psychologist and, currently, a principal adviser in the Office of the Chief Psychologist. His interests include reducing violence, programme evaluation, group therapy, young offenders, leadership, staff development, and science fiction.
Dr Nick Wilson has been working as a clinical psychologist for the New Zealand Department of Corrections for the last 18 years. His current role is as the Principal Adviser, Psychological Research with responsibility for the provision of specialist training, expert witness testimony, and research in the area of risk assessment and offender management and treatment (i.e. development of the Dynamic Risk Assessment Offender Re-entry (DRAOR) and Structured Dynamic Assessment Case-Management-21 (SDAC-21) tools). Nick has a long standing interest in criminal psychopathy and personality disorder, its assessment and treatment, and has carried out research and provided clinical services and training in this area since 2000.
Introduction
The Department of Corrections provides extensive high-quality rehabilitative programmes for a number of offender groups, including moderate risk offenders in community and prison (Medium Intensity Rehabilitation Programme, Short Rehabilitation Programme), moderate risk young offenders (Young Offenders Programme), high-risk violent offenders in the community (Tai Aroha), high-risk violent offenders in prison of medium security classification and below (Special Treatment Unit Rehabilitation Programme) and their sex offending counterparts (Adult Sex Offender Treatment Programme). However, until recently there were no intensive rehabilitative options for high or maximum security prisoners, many of whom remain for long periods without treatment due to ongoing concerns about their behaviour or management. A dilemma for many of these men and the staff managing them is that their repeatedly aggressive behaviour results in the need to maintain them at the highest levels of security. This retention in maximum and high security, however, provides limited opportunities to learn the types of self-regulation skills required to sustain sufficient periods of settled or compliant behaviour to reduce their security classifications. For prisoners being released directly from these higher security environments, this does little to prepare them for the complex and unstructured environments of everyday life with rapid re-offending related to release from higher levels of security environment. The 2013 'Staff Assault Survey' (Kilgour et al, 2013) reinforced these observations with both prisoners and staff identifying the lack of formal and intensive rehabilitation available in these environments. Interestingly, when interviewed, the prisoners who had seriously assaulted staff, without exception, expressed a degree of motivation to engage in rehabilitation.
In contrast, the Department of Corrections has previously undertaken a pilot of an intensive programme for the type of offender who typically ends up in higher security environments. This High Risk Personality Programme (HRPP) was delivered in three phases in a high/medium security environment at Waikeria Prison for a period of 11 Months (44 weeks) during 2007. Participants were selected for their high-risk status, relatively high rates of institutional misconduct, severe personality disturbance, and high levels of case complexity. Eleven of the 12 participants completed the programme with significant reductions in institutional misconduct during the therapy period and subsequent placement across the prison estate (Wilson & Tamatea, 2013). Custodial staff involved in the programme generally reported across the board improvements in participants' conduct, compliance and attitude during and following the programme, with 80% reducing their security classification over a six month follow-up period.
Since 2007 the need to provide specialised programmes for the high/maximum security prison has not abated. If anything, ongoing serious assaults on staff and other prisoners have helped to maintain a consistent cohort of prisoners in high and maximum security. The presence of this disruptive group has been one of the drivers for the significant work undertaken over the last three years to improve staff safety and decrease workplace violence. As such, the development of intensive programmes for this relatively small but high-risk, high-need subset of prisoners is regarded as a priority in the provision of a pathway to improved emotional regulation, behavioural stability, and reduction in security classification for these men. Successful transition for these prisoners to lower security placements will in turn provide greater access to alternative rehabilitative options in the lower security environments across the prison estate. The access to comprehensive rehabilitation options is necessary to address the range of dynamic risk and reintegration needs that such high risk offenders present with, in order to 'test' behaviour change and ultimately to reduce recidivism risk.
The re-build of Auckland East Prison which is currently underway and due to be completed over the next three years has highlighted the opportunity to provide a safer and more conducive environment for the delivery of effective rehabilitation programmes for maximum security prisoners. Thus, the opportunity was ripe to develop and trial programmes that are suitable to the complex needs of these prisoners. Similarly, senior staff at Christchurch Men's Prison identified a similar gap in programmes available within their high security environment and an institutional readiness to remedy this problem.
The opportunity to trial a rehabilitation programme for high/maximum security settings across the two environments during similar time periods provided a number of unique opportunities, including:
- Developing staff capability and co-support systems for the programme in more than one prison site, to help reduce the isolation of staff working with very high-risk, high-need prisoners, and enhance sharing of information between staff around delivery challenges.
- Helping to further develop cross-site strategies for the management of particularly difficult prisoners (i.e., because of the relatively few high-security and above classification environments in New Zealand) many of the prisoners concerned are known to, and rotate across, Auckland and Christchurch prisons.
- Being able to examine the relative utility of the programme across more than one physical environment with differing operational needs (e.g., programme space, delivery models such as small and medium sized groups, and unit configuration) and subsequently build in resilience for application
in different settings. - Successful delivery of the programme across the sites should provide added confidence in the ability of the therapy to reliably address violence for a high-risk, high profile prisoner group.
Prison managers provided strong support for the implementation of a suitable programme at both sites. The project therefore developed an ambitious set of deliverables and timeframes for the 2014 calendar year, including design, delivery, and evaluation of a High Risk Personality Programme-Revised (HRPP-R) at two prison sites (Auckland and Christchurch). Below we summarise outcomes for Phase 1 of the first three cohorts of programme participants - 18 men - over this period.
Description of the HRPP-R
The structure of the HRPP-R is closely aligned with the 'domain model for personality treatment' developed by Professor John Livesley (2012). This model outlines a framework for an evidence-based approach to conceptualising personality dysfunction to understand interpersonal behaviour, tailoring treatment approaches based on these conceptualisations, and selecting appropriate treatment methods to structure therapy based on general principles of therapeutic change. This targeted intervention aims to translate into direct and positive outcomes for the men participating within the HRPP-R programme. Expected outcomes are improved emotional control and behavioural stability, reduced aggression, fewer misconducts, and ultimately sustainable reductions in security classifications allowing safe placement in lower security settings. Professor Livesley's model takes a phased approach to treatment that assumes personality change occurs in the context of the therapeutic relationship, which needs to be firmly established at the early stages of treatment. The core therapeutic principles underlying this model include:
- Establish and maintain a structure and frame to treatment.
The structure and frame (focus) for the treatment has to be clear and transparent, with 'nothing hidden'. Structure has multiple parts, including the environment, schedule of sessions (programme & prison management, supervision, behaviour rules etc), and therapeutic approach (empathy, genuineness, and positive regard). The key frame or focus is on personality (patterns of behaviour) and how these impact on participants' current and future antisocial behaviour, especially where it prevents achievements of prosocial goals.
- Build and maintain a collaborative relationship.
The participants need to see the therapists as helpful and themselves as accepting of help. Both sides need to work collaboratively and have a working alliance to achieve the shared goals for the participant. The key element is collaboration. Therapists facilitate optimism and realistic hope and provide education and information on linking thoughts, feelings, and behaviour and on what personality is and how it links to problematic behaviours. But overall it is a joint search to arrive at understanding/insight. When collaboration comes under challenge, an expected condition in treating this group, then all efforts are made to repair the relationship and to learn from the experience.
- Maintain consistency.
It is important that both the therapists and participants practice consistency. It is acknowledged that participants in the past likely experienced relationships that have lacked consistency or were unpredictable. Therapists will keep the focus on the programme goals by ensuring these are clear, and also by managing negative behaviours that could sabotage collaboration. The programme has limits on what it will cover, to avoid becoming 'side tracked' from the goals of addressing current problematic behaviour.
- Promote validation.
This means that therapists provide experiences in the programme that will validate/support the participants' ability to change their behaviour. Participants are encouraged to try new approaches that bring better outcomes for them. Validation also means that the therapists listen to the concerns and experiences of the programme participants and will recognise areas of their success and competency.
- Build motivation.
Motivation to engage in treatment and to change long-standing behaviours is expected to fluctuate in the programme but motivation becomes a focus of therapy when it becomes low. Engagement in treatment, motivation and the treatment alliance are linked. So the programme provides experiences to build motivation through identifying realistic hope, addressing participants' concerns, and making the goals of therapy very clear.
- Encourage self-observation and self-reflection.
Most treatment involves some reflection on personal experience. While participants will experience things with some intensity, their reactions tend to be automatic, without conscious thought, with little time in the moment for self-reflection. The programme seeks to assist participants to move from a focus on the moment to seeing their experiences and situation in a broader context. Therapists educate the participants on a range of approaches to better understand thoughts, feelings, behaviours, and patterns in their reactions. This is expected to improve the ability of participants to manage emotions, and to recognise that some thoughts are unhelpful to achieving their personal goals. The programme wants participants to become curious about their own thoughts and behaviours and, indeed, their personality.
Based on these principles and the broader Livesley framework, the HRPP-R programme is designed to be delivered in three flexible phases to ensure individual needs are addressed. The three phases are (1) Focus on Safety, Containment and Engagement; (2) Control and Regulation and Exploration and Change; and (3) Synthesis: Construction of a More Adaptive Sense of Self and Identity. Each phase of the HRPP-R is delivered over three to four months with a break of two to four weeks between phases with completion of all three phases taking 10-11 months. Therapy is delivered in a group and individual format, with three group-based weekly sessions of 2-2.5 hours and a one hour individual session each week for each participant. Some prisoners may complete all three phases due to their retention in a high security setting, but for most, completion of phase one or the first two phases only may occur. The rationale behind partial completion is that some of the participants will be able to successfully complete a pathway out of the high security placement and thus can access existing rehabilitation initiatives to address the remaining HRPP-R areas (e.g., completion of a Special Treatment Unit Rehabilitation Programme (STURP)).
The HRPP-R therapists are all experienced department psychologists from the Auckland North psychologists office and the Christchurch psychologists office who are supervised in the pilot sites by the authors who developed the programme. A pivotal component in the delivery of the HRPP-R is that it is a team approach with custody staff involved in daily monitoring the prisoners' behaviour outside of therapy using the Dynamic Assessment Situational Aggression (DASA; Ogloff & Daffern, 2009) and in reinforcing the programme materials, and case management assisting in using the HRPP-R to progress prisoners? pathways.
How did the participants do?
In reviewing Phase 1 of the HRPP-R we examined results from exit interviews conducted with a sample of Phase 1 completers; analysed DASA results on men attending the Auckland programme; compared prisoner misconducts and incidents in the six months pre-programme and subsequent to first contact with the programme; outlined observations from supervision of therapy staff and other formal and informal sources of information around treatment outcomes.
Exit interviews
Exit interviews were offered on a voluntary basis to 11 of 14 Phase 1 prisoner completers across Auckland and Christchurch prisons following the first cohort completions. One individual had already left the unit to attend a STURP by the time of interview and a further two individuals were unable to be seen due to time constraints. Ten of the 11 participants completed the exit interview process. Results from the 10 valid exit interviews were collated and summarised with key observations and patterns outlined narratively below.
Overall, participants rated Phase 1 of the HRPP-R as average or better on a 6-point scale anchored from 'Didn't like at all' (1) to 'It was great' (6) with an average rating of 4.8. All men indicated that they would recommend attendance to others in their unit, citing a range of reasons including self-improvement related reasons to decreasing boredom and lowering security classifications. Most similarly rated the programme highly in terms of goals to manage their behaviour within high/maximum security (mean = 4.5); reduce security classification (mean = 4.1) and prepare them for further treatment (mean = 4.6).
In regards to improvements in programme content, a range of suggestions reflected the idiosyncratic interests of group members with only one topic reported more than once (4 times); summarised by a theme of spending more time on 'goals and values' promoting change. Similarly there were no themes around aspects of the programme that participants found difficult. Most men had either struggled to stay in the programme at some point during the 10-weeks and/or - in contrast to reality - had believed they were at risk of being prematurely removed. However, typically men were pleased that they had persisted with the programme, often citing that the peer support within the programme helped to maintain their commitment. Indeed, a deepening of relationships with co-members was noted by almost all participants, even though a degree of suspiciousness and lack of trust of others was described by many as a personal challenge, particularly early in the programme. Despite these trust issues, most men thought that others in the group (including facilitators) handled their personal information and disclosures with respect and appropriate confidentiality, and that the rules of the programme were generally respected. An exception to this was a number of men - in the Christchurch cohort - acknowledging that they tended to push the boundaries around group rules and attendance. These men in their feedback encouraged facilitators to be more directive and enforcing of group rules. Despite this, most of the participants thought that the group had acceptable structure, including the length of the programme, and group and individual sessions.
Therapy staff were generally rated highly in terms of competence, genuineness and trust, with effective ongoing therapeutic relationships. A number of men noted that they were appropriately challenged by facilitators as to attitudes and behaviour. Custody staff were rated somewhat more poorly in terms of their genuine interest and support for the men in their problems and changes. However, participants generally saw the custody staff as 'fair' in their interactions and typically there was at least one staff member who they perceived as a good support during the programme.
In terms of how the men perceived themselves as having changed while on the programme, the exit interviews probed for more general change and also specific behaviours around handling conflict. More generally there were themes of increased awareness (e.g., about personal thinking and behaviour, the perspectives of others, and behavioural options); and being less reactive and angry. Strategies to manage conflict included a broad range of emotional and behavioural responses with many men citing more than one approach. Several men noted a sense of internalised reduction in emotional reactivity (e.g., 'people said I'm different - I don't sweat the small stuff'; 'I'm less angry now'; 'my mindset's changed'; 'the officers are saying I don't get angry as much').
Dynamic Appraisal of Situational Aggression (DASA) results
In order to bring some objective and independent analysis to the self-report of programme participants, custody staff were trained in the rationale and administration of a measure used to predict aggression over the short-term. The DASA was intended to be used on a daily basis for all participants during the Phase 1 trials and was part of broader evaluations of the use of this measure across a number of Department of Corrections' sites (Kilgour & Wilson, 2014; Kilgour & Wilson, 2015).
The DASA is described as "efficient and should take less than five minutes to complete" (Ogloff & Daffern, 2009, pg 19). Scoring is based on the presence or absence of objective behavioural descriptions of seven items (i.e., irritability, impulsivity, unwillingness to follow directions, sensitivity to perceived provocation, easily angered, negative attitudes, verbal threats) over the 24-hour period prior to rating. The occurrence of aggressive behaviour (verbal towards people, or aggressive towards objects or people) is also recorded for the target period. Depending on the number of items rated as present, individuals are allocated a 'low', 'moderate', or 'high' level of risk for further aggressive behaviour over the next 24-hour period and staff are encouraged to share these risk ratings and the relevant items with the next available shift. Ultimately, the DASA assesses a state of irritability and disagreeableness with this state preceding most acts of aggression irrespective of mental disorder (personal communication, Professor Michael Daffern, October 2012).
DASA scores were collated consistently by staff at Auckland Prison during the first Phase 1 cohort and Figure 1 shows examples of composite scores by week for one participant, which was representative of the other five participants. This shows the presence of any DASA item on a given day within any particular week of the programme, rather than total DASA score on any given day. It is notable that no individual participant scored more than '2' (i.e., the presence of more than two items suggesting 'Moderate' risk for violence in the next 24-hours) on any given day and that by week seven of the programme there were no items observed for any of the participants. Perhaps coincidentally, week six of the programme introduced emotional control strategies for participants. Regretfully, custody staff did not reliably complete DASA recording for any length of time at the Christchurch site and so comparable scores were not available and we were unable to test if there was a similar improvement with emotional control in week seven. However, from the limited results obtained on the first cohort from Auckland, by the seventh week of the programme, participants there were generally settled with no evidence of notable concerns in their unit behaviour.
Presence of DASA item by week: Client A
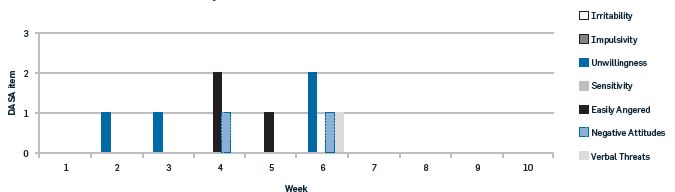
Figure 1.
Presence of individual DASA items by week for Client A
Incidents and misconducts
In an attempt to obtain an objective and independent measure of demonstrable behavioural change, official records of misconducts and incidents (events) were examined for two time-periods: (1) the six months prior to the first contact with HRPP-R programme staff (typically the pre-programme assessment interview); and, (2) the time elapsed since this first contact. As at February 2015, these periods were relatively equivalent for the 18 men who had attended Phase 1 of the programme, with a total of 3,276 days (6 months each) for the pre-programme period and 3,884 days following the first contact with therapy staff (an average of approximately seven months per programme participant).
All recorded misconducts and incidents for each participant were reviewed individually for these periods. When an incident and misconduct referred to the same event, the event was recorded only once as a misconduct, to avoid double-counting. Events were classified by type: 1) violence; 2) property damage; 3) contraband; 4) non-compliance; 5) substance related; 6) other. Violent events included any physical or verbal aggression against another prisoner or staff member, including behaviours such as verbal threats, abusive language, accusation of threats, inciting violence, and spitting.
Table 1 displays the number and type of event across the two time periods. Figures 3 to 5 display aspects of this data visually. Overall there was a 34.4% decrease in the number of events recorded for the HRPP-R participants. Although there were rises in two categories (contraband and non-compliance) these were largely in the 'incident' rather than 'misconduct' category, reflecting behaviours of a lower level of seriousness. One collective event, whereby several programme attendees in Christchurch attempted to bring food back into the unit following their Phase 1 graduation, accounted for five of these incidents.
Of note is the almost 70% reduction in violent events. Looking at violence against staff specifically, this includes a reduction from 14 assaults (4 assaults and 10 violence threats) against staff during the pre-programme phase to no assaults and two threats against staff (an 86% reduction) following first contact. The number of weeks when programme participants were involved in no recorded events more than doubled from four weeks (in the six months pre-programme) to 10 weeks in the six months from initial contact. Similarly the number of weeks with no violence-related events went from nine to 21 weeks in the same time frame. Thus, not only was there an overall reduction in events, the number of 'event free days' more than doubled during the programme period.
Drilling down to individual results for programme participants, for four individuals the rate of events actually increased from the pre-programme to post-first contact period. One man had one extra event but a reduction from one to nil violent events; one went from four to six events with a reduction from one to nil violent events; one went from three to six events but a reduction from one to nil violent events; one went from four to nine events but a reduction in violent events from three to one. All of these men were from the Christchurch programme, perhaps reflecting the greater opportunity to engage in problematic behaviour within the less controlled environment of high security compared with maximum. Although it is gratifying that violent events still declined for each of these men, they still reflect an ongoing management concern and highlight the degree of complexity and difficulty working with such prisoners.
Table 2.
Misconducts and incidents for HRPP-R participants, pre-programme and following first contact.
|
Description |
Misconduct |
Incident |
Totals |
Misconduct |
Incident |
Totals |
Change (totals) |
|
Violence |
23 |
5 |
28 |
4 |
5 |
9 |
-67.9% |
|
Property damage |
2 |
4 |
6 |
5 |
1 |
6 |
0% |
|
Contraband |
10 |
1 |
11 |
10 |
7 |
17 |
+54.6% |
|
Noncompliance |
5 |
1 |
6 |
4 |
3 |
7 |
+16.7% |
|
Substance related |
7 |
0 |
7 |
3 |
0 |
3 |
-57.1% |
|
Other |
2 |
4 |
6 |
0 |
0 |
0 |
-100% |
|
Totals |
49 |
15 |
64 |
26 |
16 |
42 |
-34.4% |
Misconducts & Incidents by Type
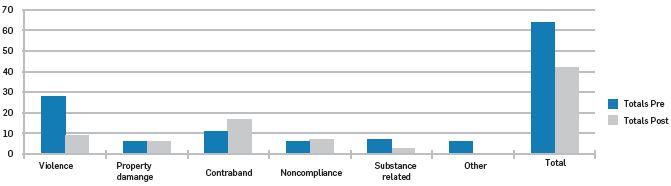
Figure 2.
Summary of Misconducts and Incidents pre-programme and following first programme contact.
Number of Incidents/Misconducts by Week
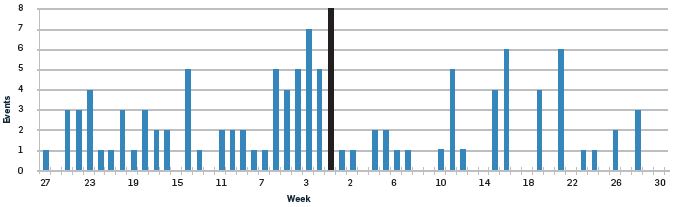
Figure 3.
Misconducts and incidents pre-programme and following first programme contact by week for all participants (red line signifies first contact with programme staff).
Violent Misconducts/Incidents by week
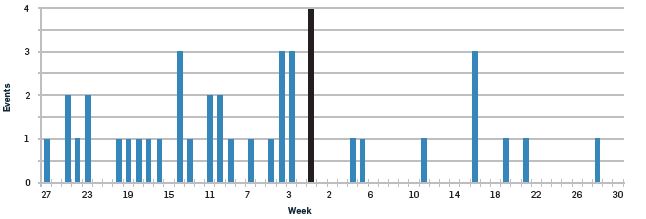
Figure 4.
Violent misconducts and incidents pre-programme and following first programme contact by week for all participants (red line signifies first contact with programme staff).
Supervisory observations
Turning to less objective observations of programme outcome, the authors engaged in weekly clinical supervision of HRPP-R therapists to support the implementation of the programme. None of the following comments should be ascribed to any particular therapist or group participant. However, some general observations are worth reflecting on:
- As expected by virtue of their prison placement and institutional behaviour, programme participants evidenced a high degree of personality pathology in their pre-programme psychological testing results and this was reflected within their behaviour, particularly in - but not confined to - early group stages.
- It is noted in the literature that individuals with similar personality pathology are natural rule breakers/challengers, often with subsequent
poor adaptation to high rule or inconsistent rule environments. - Levels of challenging behaviour - sometimes referred to as 'storming' in the group therapy context - were very high in the early weeks of group, with facilitators having to work hard to balance the need to establish clear boundaries to contain inappropriate behaviour but also build trust and a strong therapeutic foundation. For example, participants challenged therapists' competency, abilities, commitment, boundary setting, and management of personal disclosures (including safety issues).
- During the early stages there were doubts about the ability of many participants to participate effectively in the group environment and their willingness
to engage. However, perhaps surprisingly, the persistence and flexibility of all, contributed to no voluntary exits during any of the three Phase 1 groups. - Although there were similar patterns for many participants in the measurement of their personality pathology (e.g., paranoia, antisociality, reactivity, poor emotional self-regulation, and interpersonal dysfunction) these were often expressed idiosyncratically, with the need to develop individualised management plans for each group participant.
- The weekly individual sessions that sat alongside the group process became useful for participants to 'debrief' from the group process, and for therapists to challenge particularly unhelpful behaviours that participants may have been more resistant to addressing in front of their peers. Individual sessions also served to enhance the rapport and speed up the engagement of participants.
- Challenges experienced in the group were moderated differently by the respective physical environments in Auckland and Christchurch prisons. For example, the physical transparent screen between therapists and group members in Auckland Prison resulted in 'storming' to be less intense but longer lasting than the open-plan group room in Christchurch. In contrast the screen and more rigid consistent rule-based environment of the maximum security regime in Auckland assisted earlier and more effective boundary setting and group rules than in Christchurch.
- Changes with these groups of men are often limited, gradual and tenuous but also could sometimes be profound. As supervisors at some physical and emotional distance from the respective settings it was notable that, in working with these men on a daily basis, therapists sometimes lost sight of the positive movement in attitude and behaviour compared with the early stages of the programme.
- It is notable that at both prison sites there were examples of participants actively working to support one another through difficult periods of the programme. For example, prison staff in Auckland observed one prisoner was actively encouraged by others on the programme to manage a period of difficult interactions with his partner in a less hostile manner than he had in the past; Auckland participants were observed to assist each other in the completion of homework; Christchurch participants reported actively avoiding gang leaders in their unit leading up to the start of the programme so that they could avoid being instructed not to attend; Christchurch prisoners argued to staff attending the Phase 1 graduation that being housed on the same landing - despite gang differences - would have assisted their engagement and motivation for the programme.
In summary to this point, HRPP-R participants are complex individuals with significant personality issues and histories of difficult behaviour both in and out of prison. Within this context the skill of, and support given to, therapists is critical to the success of the programme and retention of participants. The degree of conflict and challenge for therapists within these groups is very high. The ability to manage this is supported by:
- Selecting therapists who already have experience working with high and complex needs, and correctional clients.
- Therapists attending specialist training in personality pathology and thoroughly integrating this into their everyday assessment and practice.
- Regular supervision containing deliberate components on managing group process and relationships.
- A transparent and consistent frame or model to support supervision and clinical practice. Our experience of implementing the Livesley model - as described above - suggests this was a 'good fit' with the needs of both group members and therapists. This frame also helps therapists to understand and 'depersonalise' the significant and ongoing challenges (including intermittent hostility) experienced in their work with these clients. In particular they are more able to stay more objective, retain realistic expectations about change, make 'safe' therapeutic and ethical decisions, and consequently get through the daily challenges.
- A team approach to managing the HRPP-R programme. This team not only includes facilitators and supervisors but the principal psychologist (to work with custody in identifying and reducing administrative issues and barriers), the prison director (for higher level support and endorsement) and custody staff (to help manage practical day-to-day requirements, objectively observe prisoner behaviour, manage conflict and safety issues in the unit, and support incremental changes in prisoner behaviour).
Placement outcomes
Although relatively early in the scheme of long-term outcomes for programme participants, a key goal is to have participants reduce their security classifications due to improvements in their behaviour, and transition to environments that are able to provide offence-focussed rehabilitation and reintegration. At this early stage and following the Phase 2 groups, several men have reduced their classification and transferred out of the HRPP-R units. At the time of preparing this article three of the Christchurch men have successfully transferred to lower security settings; one was moved but returned to high security, and a further man was in the process of transitioning. In Auckland three men have transitioned out of maximum successfully with a further individual transferring but failing to successfully adjust. Most of the men remaining in high security (both at Auckland and Christchurch) have continued to engage with Phase 2. For the men who did not begin Phase 2 or withdrew, one has returned and the therapists continue to seek ways of maintaining their engagement in the change process through intermittent individual appointments.
In conclusion
The HRPP-R Phase 1 programme was successfully delivered across two very different high security prison settings by Corrections' psychologists following the session material guidelines. The treatment materials and intervention approach appear to match the therapy needs of the HRPP-R participants and to address the anticipated institutional and personality responsivity issues.
In terms of the therapy goals for Phase 1 of the HRPP - Safety, Engagement, and Containment (of acute emotions) - there is some early evidence that the programme has been successful in addressing these during therapy. These changes should be considered tentative and limited at this stage of the programme. However, they provide an indication that the HRPP-R is both able to be run effectively within maximum and high security environments, across different sites, and with some of the most difficult and intransigent prisoners in the country.
References
Kilgour, G., Paramo, R., & Wilson, N. J. (2013, January). Staff Assault Survey Project Report Summary. Office of the Chief Psychologist, Department of Corrections, Wellington
Kilgour, G., & Wilson, N.J. (2015). The Dynamic Appraisal of Situation Aggression (DASA): An updated report on the trial use of the measure. Office of the Chief Psychologist, Department Of Corrections, Wellington.
Kilgour, G., & Wilson, N.J. (2014). The Dynamic Appraisal of Situation Aggression (DASA): A report on the trial use of the measure. Office of the Chief Psychologist, Department Of Corrections, Wellington.
Livesley, W.J. (2012). Integrated treatment: A conceptual framework for an evidence-based approach to the treatment of personality disorder. Journal of Personality Disorders, 26(1), 17-42
Ogloff, J.R.P., & Daffern, M. (2009). The Dynamic Appraisal of Situational Aggression: Inpatient version - adult. Centre for Forensic Behavioural Science, Monash University, Victoria, Australia.
Wilson, N. J., & Tamatea. (2013). The high risk personality programme: An experimental approach to treating psychopathic prisoners. Psychology, Crime and Law. DOI: 10.1080/1068316X.2013. 758994