Pursuing consistency: multiple sites; one drug treatment approach
Edward Kitchin
Project Manager, Odyssey (Auckland)
edwardk@odyssey.org.nz
Author biography:
Ed has over 10 years’ experience operating alcohol and other drug (AOD) services within correctional settings, initially working in the UK on the innovative Drug Intervention Programme (DIP), which directed adult offenders into drug treatment. Moving to New Zealand in 2010, he has worked in Drug Treatment Programmes (DTPs) in prisons for the last seven years. He joined Odyssey in 2016 to oversee DTP implementation at three Department of Corrections’ sites.
Odyssey has been running a Drug Treatment Programme (DTP) at Auckland Prison since 2010. In early 2017, this contract was renewed and Odyssey was awarded two further DTP contracts: at Spring Hill Correctional Facility in Waikato and at Christchurch Prison (in partnership with Odyssey House Christchurch).
Implementing an intensive prison-based drug treatment programme is not without its challenges. Of course these challenges increase exponentially with the number of sites being established – each site has a unique culture, context and population.
While we valued the diversity across the sites we were operating in, we were conscious of the need to establish consistency in our approach and commonality across programme aspirations, content, processes and procedures.
We were keen to avoid the risks that might arise should programmes evolve locally and independently. These include the potential for:
- Confusion about our treatment approach and model of best practice
- Lack of clarity for prisoners and Corrections staff about the nature and practice of an Odyssey DTP
- Disparate and/or irregular quality monitoring
- Version control and updates to systems and processes managed in an ad hoc or cumbersome fashion.
In the light of these risk factors, maintaining consistency was top of mind throughout the implementation process and, indeed, has been an ongoing consideration within the day-to-day operations at each location.
To support these efforts, we developed a tool that would provide a solid foundation for the implementation and subsequent operation of the three DTPs. This tool has become known as the “Quality Wheel”.
The Quality Wheel was developed and trialled across the three sites throughout 2017. The tool has been instrumental in driving the successful implementation of new models of service delivery across each location.
What is the Quality Wheel?
The Quality Wheel is a cloud-based tool we designed in-house that operates much like a front door or “portal” to all aspects of the programme. It was designed to provide a simplified interface to a complex system. Staff can access the wheel via a simple web link; no sign-up is required. They are then able to view and interact with the wheel. It is hosted in software called “Lucidchart” which enabled us to create our own base template from scratch resulting in a visual that communicated a clear message.
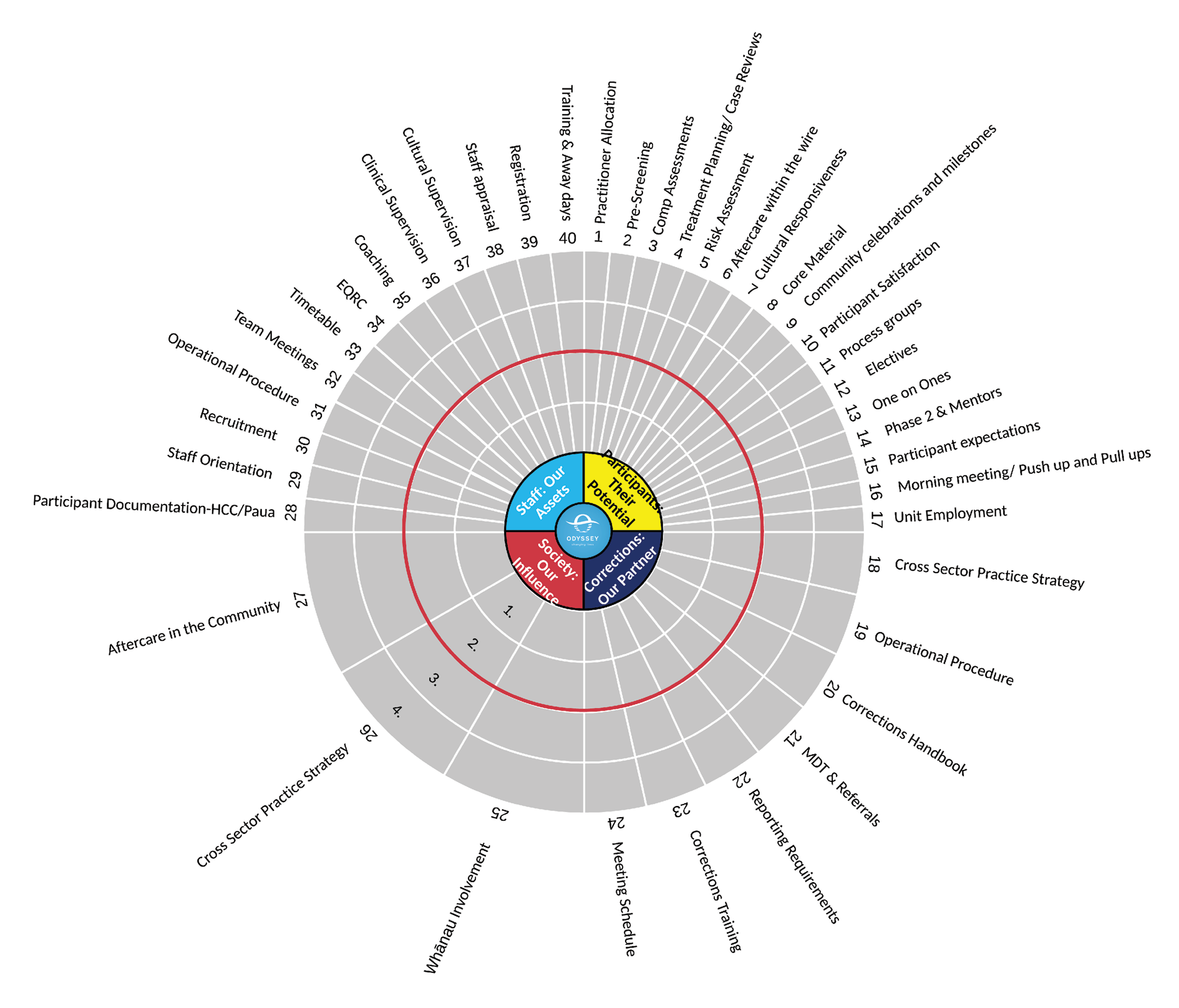
The wheel evolved along with the implementation process as we considered how to pull together the variables. What we ended up with looked like this:
Odyssey Drug Treatment Programme Quality Wheel (2017)
How it works
The Quality Wheel achieves consistency by targeting four core areas:
- Fostering collaboration
- Reinforcing the vision
- Developing clear, accessible resources and systems
- Monitoring quality.
Fostering collaboration
Collaboration throughout the implementation process was essential to develop a shared vision and maintain consistency in our approach. We initially focused on collaborating with staff at the coalface to ensure resources and processes were both relevant and responsive to their needs, and the needs of participants.
This also facilitated greater acceptance of the service vision, policies and processes by the wider staff network, which in turn secured successful implementation.
We used cloud-based* documents that could be accessed by clicking the relevant area of the wheel. Every project document was accessible through the wheel and every document was set up to allow suggestions and comments by staff.
In this way, staff were able to provide real-time feedback based on their (and participants) actual experience of using materials and resources within the DTP. For example, if a staff member, while running a group, noticed that instructions were too complex, or language did not suit a given situation, or an additional step might be needed in an exercise, they were able to comment within the master document.
An automated email would then alert the project manager, who would be able to accept or reject the suggestion within minutes. Thus, content and processes have evolved dynamically in response to staff and participant feedback.
(*To maintain data security, the cloud was only used for content and policy, not to store any personal client information.)
Reinforcing the vision
We can sometimes lose sight of the big picture as we become focused on the day-to-day practicalities of project implementation. Ultimately, our DTP programmes are about changing lives and keeping this fact at the forefront both motivates staff and provides clarity in decision making.
The wheel was designed to visually convey how each aspect of the programme contributes to this central vision. Each spoke of the wheel points towards the greater purpose. The hub of the wheel is broken into four quadrants:
- Participants: Their Potential
- Corrections: Our Partner
- Society: Our Influence
- Staff: Our Assets.
These quadrants, which represent our aspirational values for the DTPs, are described in greater detail when users click through to the supporting documents. However, we believe they also speak for themselves in the context of the programme and the business of changing lives.
Consistency in the detail of the programme needed to go hand-in-hand with a clear view of the big picture, and the wheel provides a constant reminder of what we are about.
Developing clear, accessible resources and systems
While we already had a DTP running at Auckland Prison, we still needed to update our resources to reflect new contract specifications. This also provided an opportunity to consider whether there were additional changes we might wish to implement, so we reviewed and rewrote the entire syllabus.
We temporarily moved our document cache to the cloud-based platform and made every effort to ensure the layout was intuitive and clear. This allowed us to direct users to the current versions of all documentation, minimising confusion around version control and ensuring outdated versions were not being used. It also meant staff new to Odyssey did not need to familiarise themselves with potentially complex file paths on shared drives.
We also provided a master list of documents to support navigation of the various elements of the programme.
Monitoring quality
Perhaps the most important function of the wheel was to provide a visually striking and intuitive quality monitoring and assessment tool. At specified intervals, the clinical managers at each site are required to review the 40 spokes of the wheel within their programmes and score them appropriately.
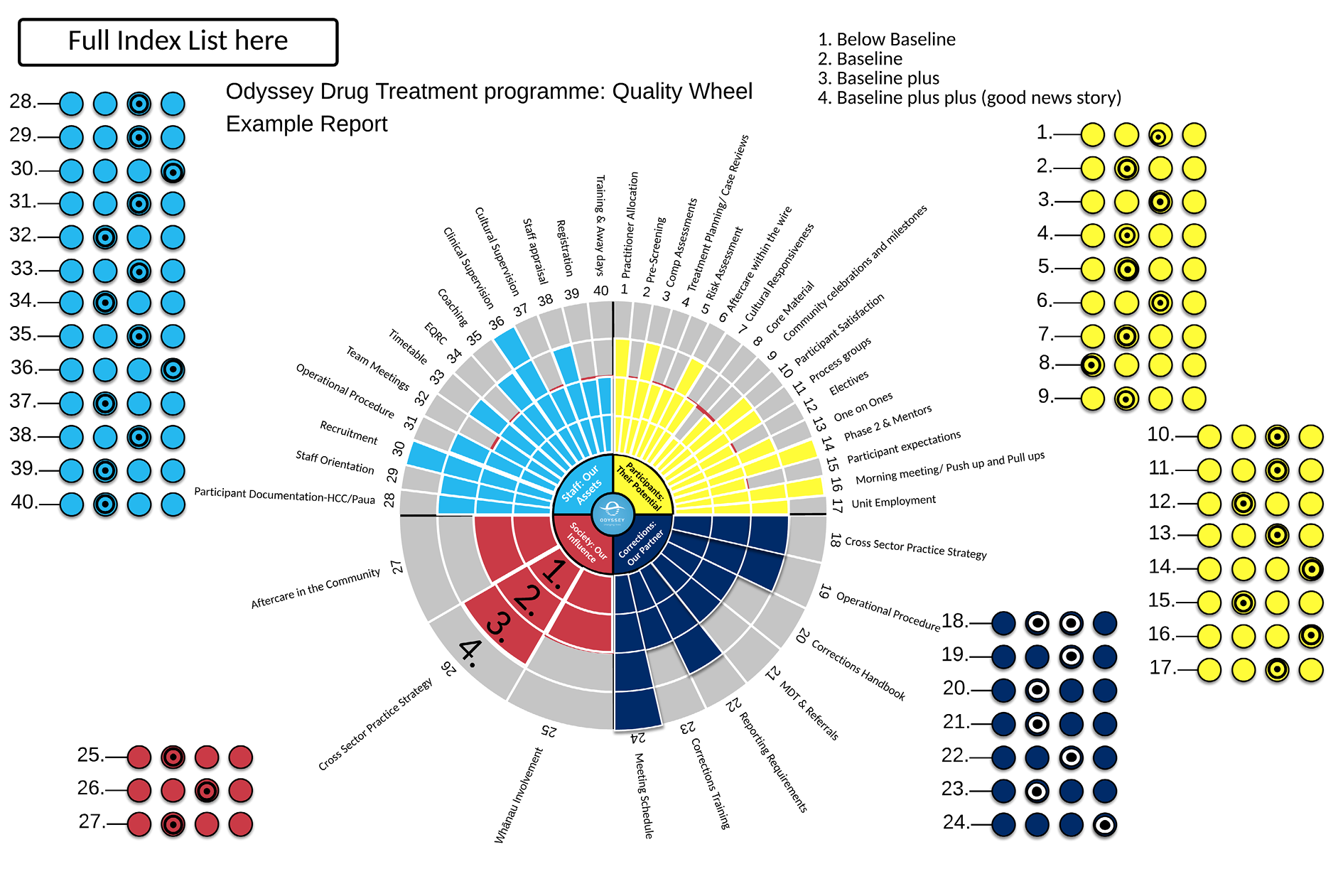
The basic principle when assigning a score to each spoke is as follows:
Score of 1 = Below baseline
Score of 2 = Baseline (meets contract specifications)
Score of 3 = Baseline plus (meets two or more additional criteria)
Score of 4 = Baseline plus plus (good news story).
We developed a scoring guide that gave specific criteria for each of the 40 spokes. See example below for spoke 8 “Core Material”:
8. Core Material | |
|---|---|
Monthly Baseline – Records indicate all DTP participants have experienced 3 hours of psychoeducational material per week. (HCC see client assessment report ‘clinical attendance’). Evidence of exceeding this (Baseline +), would include 2 or more of the following -
To qualify for level 4 (Base line ++) provide a good news story | Good news Story?: |
Score - 1-4 ☐ | |
Once a score for each of the 40 spokes has been ascertained, managers can then colour their wheel by clicking the dots adjacent to it, reflecting this score.
This allows each site to illustrate at a glance the performance of their units over a given time period. (i.e. 1 = one layer of colour, 2 = two blocks up to four where the whole spoke is coloured (As in spokes 14,16 and 24 below).
Odyssey Drug Treatment Programme Quality Wheel (Example Report)
Initial evaluation
Ten months in, staff feedback has been very positive and the uptake has been relatively smooth, particularly in regards to accessing the content through the wheel.
The wheel has been particularly valuable over the set-up phase, connecting the sites and enabling us to learn from one another. This has led to valuable discussions at our clinical steering group meetings.
The wheel has also proved useful for connecting staff with practical guidance and the thinking that lies behind each process. For example, the pre-screening spoke opens the page pictured below, which outlines the tasks, the purpose and the relevance to contract specifications/reporting requirements.
| Pre-Screening |
|---|
Monthly Baseline - All participants in the most recent intake had direct contact from Odyssey staff (or evidence of attempts), before starting the programme - ideally ahead of their arrival into the unit. (either face to face or via telephone), and undertook the Pre Screening Form. Evidence of exceeding this would include 2 or more of the following -
|
Purpose of Pre Screening assessment
Produce and assessment report in the APF format - (Activity Progress Form)
The APF needs to be submitted to the DTU schedulers, no more than 5 days after the assessment. |
This has allowed practitioners to gain more insight into each process, including how it links into broader Corrections systems. For prisoners, this has resulted in receiving clearer, more consistent information from Odyssey. This has enormous value as it sets up the expectations clearly ahead of arrival, lessening the potential for culture shock and increasing the likelihood of a smooth and positive transition. Ultimately this increases the retention rate and therefore the efficacy of the entire programme.
The quality monitoring/reporting function of the wheel has taken some time to establish and embed. We are still working through how we can enhance the measurement and evaluation aspect of the wheel going forward.
One of the hazards we all face is inadvertently adding to the administrative burden for staff. While the tool increases efficiency in some regards, it does not negate or eclipse the necessity to undertake the established data entry or quality monitoring tasks. Given the experimental nature of the tool, the quality monitoring aspect is not yet fully integrated organisationally and clinical managers are still required to run the standard quality audits in addition to this tool.
A further aspect to consider is the nature of cloud hosting. The enormous benefits of using the cloud must be balanced against the risks, which include: staff being put off by more passwords and usernames, the potential for intellectual property disputes, potential difficulties accessing data when it is not stored on your own servers, unreliable internet connections with insufficient bandwidth and the big one – security.
We moved with caution in the light of these risks. For example, we ensured that no personal/client information was hosted in this space. While there are no quick answers to these concerns, the tide is turning across all industries towards cloud-based software. Those of us working in the “people industry” have a number of additional considerations to take into account. However, we risk being left behind if we move too slowly and there are some very robust risk mitigation strategies we can employ.
Conclusion
The Quality Wheel has helped Odyssey ensure consistency of implementation across its three DTPs.
However, it must be noted that while the use of technology has allowed us to communicate in new and more efficient ways and support a shared purpose and understanding of a common approach, we recognise that not all processes or resources will suit each site all of the time. Similarly, innovation can be stifled in the pursuit of consistency, and care must be taken to ensure communication and feedback channels foster staff initiative and experimentation where appropriate. Cookie-cutter solutions may maintain consistency but they also lack personality.
The wheel, like any tool, needs a skilled operator, someone to faithfully maintain it with care and understanding. This includes maintaining good relationships, meeting regularly and allowing flexibility around the model. These factors are also essential to success.
The wider Corrections estate is broad and diverse – the prisoner make up, regional differences, site characteristics and contexts all contribute to the distinct cultures found at each facility. While this can pose a challenge for centralising systems, it is also to be celebrated, as it fosters diversity for a diverse muster.
Investment in systems is not enough in itself – it must go hand-in-hand with an acceptance of the cultural differences at each site and a willingness to empower local decision making. When organisational leadership invests in its relationships with staff on the floor, this will empower staff to invest in the relationships that really matter: those with the prisoners.